The main problem with Knee Pain is that it very quickly interferes with the correct function of the surrounding, supporting muscles. This causes a ‘Catch 22’ effect:
Pain in the Knee (from whatever source) -> Muscles surrounding the knee become Inhibited and don’t Activate when they should -> Muscles quickly become Weak from Disuse -> Reduced Support for the Knee -> More Strain on the Knee Structures -> More Pain
Accurate Diagnosis of the Problem
Most people that come to see us have Googled their symptoms and many have a good idea of what might be going wrong. Considering the amount of self-help information out there, you might think that there is little need for a physio input – you’d be wrong, as is testified by the number of clients with knee pain that we see and help on a regular basis!
The problem with using ‘Dr Google’ is the ‘one size fits all’ approach. It is imperative to find out the main contributions to the specific pain cycle for each individual, to be able to devise an effective programme of advice, corrective exercises and therapy.
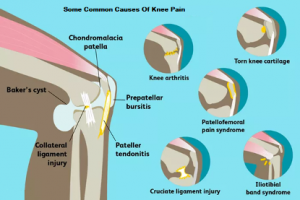
Knee Pain can come from the knee joints, the surrounding muscles, tendons or ligaments but it can also come from further afield – the hip joint or the lower back for instance. It can be due to many factors: your biomechanics, how you are standing, walking and moving, or from that injury you had a while back that you thought you’d got away with. It’s your unique history that makes you different from everyone else. This is where we come in!
A physiotherapy appointment for a client with knee pain goes through, in depth, the history of this problem so far, how it is affecting you now and what it is stopping you from being able to do. It also goes through any other issues that you might have, your previous injury and activity history along with your general health, medication etc.
A full physical examination checks the mobility of your knees, hips and any other structure that may have been flagged up from the original history-taking. There are several specific, physical tests that check the various structures of the knee. Even in On-line Appointments, we have been able to replicate many of these tests with activities that can alert us to structural problems that may need further investigation.
Do I Need a Scan or X-ray?
Many people think that they need a scan or x-ray before they can commence treatment. In the case of trauma, where there is significant pain, or other abnormality, an x-ray and/or further tests may be required. However, in most cases that we see, there is no acute trauma; there may have been an injury, but often nothing specific or severe enough to warrant an A&E visit.
We therefore generally recommend further investigations only in those cases where our questioning or examination show up instability or other abnormality; where there has not been the progress we expected, or there has been significant trauma that was not investigated fully at the time. In these instances, we can liaise with the patient’s GP to recommend the tests that we think are necessary or can advise further referral to Consultants through the NHS. We also work with a wide network of trusted, Knee Consultants, Sports Doctors and Rheumatologists and so we can help choose the most suitable Specialist if further referral becomes necessary.
Will Wearing a Knee Support Help?
A knee support or brace can help in the early stages after an injury when the pain is severe and you need to walk or stand for periods of time. However, it does not train muscles or address the causative factors and does not help you other than giving some support. It cannot be used instead of treatment and if used for too long can encourage the muscles around the knee to weaken further as they have less work to do. Careful assessment and treatment of your knee is the key to changing and improving your symptoms.
Main Guidance for Knee Pain
In early stages, use the PRICE method – Protection, Rest, Ice, Compression, Elevation.
Once the initial pain is under control, it is generally advisable to try and move the knee as normally as possible. If you have been given some exercises or have some stretches, it is fine to start them now. The important thing to remember is that any exercises themselves should not be painful – if they are, they contribute to the pain cycle outlined at the beginning of this article. Returning to exercise should be gradual, bearing in mind that running especially, loads the joints with more than double body weight, so it is best not to commence your return to exercise with a run. Walking and cycling are lower impact activities that can be helpful to build back up function and strength.
If the pain persists beyond 7-10 days in spite of you trying to do all the right things, then you might need to book in to see us for an assessment and specific programme to get you back to your sport or activity.
What Might Treatment Involve?
As mentioned earlier, physiotherapy treatment for knee pain will very much depend on what the physiotherapist finds during the initial assessment. If, for instance, the problem relates to muscle imbalances around the knee, maybe through a sudden increase in running – treatment will be directed at stretching some tissues while strengthening others. If however, the primary problem is further away, treatment might include joint mobilisations for the spine, hip, knee or ankle. Massage and other soft tissue techniques can be used and acupuncture or dry needling is often very helpful for knee problems especially in cases of osteoarthritis. If the knee is being over-loaded, possibly though poor biomechanics, a prescription might include shoe orthotics or altered running style. Taping techniques can be helpful in some cases, in a diagnostic as well as treatment capacity by off-loading specific structures or improving muscle activation. Core strengthening exercises are often prescribed to offload pressure on the knee and other lower limb structures.
The intensity and loading of any exercises, very much depend on the capabilities of the structure, the stage of the healing cycle along with the patient’s requirements and preferences. Yet again, there is no size fits all – an elite athlete will be following quite a different rehab programme to a sedentary office-worker, even though both might have what seems like a similar knee pain. Some clients like a lot of exercises and others want a pared-down list of the basics that they can focus on. Together, we work out a programme that will be effective, feasible and attainable. Exercise software has also greatly improved the patient experience – we can email you your programme so that you have a photo or video reminder.
Finally, the response to treatment is very individual and this is where the tailored approach is invaluable. As physiotherapists, we expect to see changes relatively quickly – either a decrease in pain, and/or an increase in function. The treatment is adapted all the time, from that first meeting to ensure that progress is maintained. The aim is to correct the underlying factors to allow the body to heal and then support and facilitate this process with the right rehabilitation programme to get the client to where they need to be.